
Feb 7, 2022
Unfortunately, claims alleging failure to diagnose and treat periodontal disease top the list of legal action against dental professionals. Those subject to such litigation may find it a highly stressful experience, especially if it leads to investigation by the General Dental Council (GDC). Cases commonly involve multiple dental staff who treated a patient over several years, and many take a year or more to resolve. Settlement frequently involves large sums – over £25,000 in most cases, and often more than £100,000.
To avoid future claims related to periodontal diseases, dental professionals must follow relevant guidelines, communicate their findings with patients, and keep detailed records. Defence against such a claim is much more difficult if the patient’s records do not document relevant examinations, investigations and diagnoses, as well as advice and treatment.
UK classification of periodontal disease
Regular screening and early diagnosis are essential for managing periodontal disease and preventing tooth loss, with its consequent disabilities and health impacts. Importantly, periodontal disease can be asymptomatic even in advanced cases and is only identified by dental professionals.
To support clinicians in recognising and diagnosing the condition in general dental practice, a new international classification system for periodontal disease was agreed at the 2017 World Workshop. This was subsequently adapted and adopted for use in the UK by the British Society of Periodontology and Implant Dentistry (BSP).
UK dental professionals should refer to BSP’s UK Implementation, which classifies periodontal disease into stages based on severity (I, II, III or IV) and grades based on disease susceptibility (A, B or C).
As explained in the UK implementation of European S3-level treatment guidelines for stage I-III periodontitis, the clinical pathway for diagnosis of periodontitis includes 4 steps:
- Basic periodontal examination (BPE) screen (see BSP’s BPE guideline and Simplified BPE guideline for under 18s)
- Provisional diagnosis
- Further investigations (radiographs and detailed probing charts)
- Diagnostic statement. This includes: definitive diagnosis; extent (localised or generalised); stage and grade; current status (stable/unstable); and risk factors.
A BSP decision-making flowchart is available to help practitioners implement the classification.
Why clinical negligence cases arise
A substantial number of complaints, claims and even referrals to the GDC arise because of allegations that the treating dental professional(s) failed to examine, investigate, diagnose or properly treat periodontal disease. The usual three-year limitation period may not apply if a patient can demonstrate that they only recently learned of their condition.
Successful claims often hinge upon insufficient documentation. Even if the treating dental professional argues that they did assess, treat and inform the patient correctly, they will find it difficult to support that argument if the patient’s clinical records do not show a complete and accurate record.
Since the consequences of undiagnosed or improperly managed periodontitis may be serious, compensation pay-outs are often highly costly, including damages for pain and suffering, loss of teeth and damage to the jawbone, remedial treatment costs as well as loss of earnings. Dental professionals should be aware of the risk and protect themselves from future litigation.
Reduce the risk of damaging litigation for periodontal disease
Follow guidelines: Dental professionals can reduce the risk of being subject to a claim or complaint for failure to diagnose and treat periodontal disease by following the BSP guidelines on classification and treatment.
Perform regular screening: The BSP Parameters of Care statement emphasises that oral healthcare professionals have a responsibility to screen patients regularly for periodontal and peri-implant disease, using appropriate clinical investigations to aid diagnosis and formulation of a treatment plan.
Seek specialist help if required: Patients with periodontal diseases may be referred according to BSP guidelines for a specialist opinion to assist with patient management.
Communicate well: The BSP statement also stresses the importance of good communication between clinicians and patients. Following every assessment, dental professionals should take time to explain their findings to the patient and discuss all reasonable treatment options, obtaining informed consent where necessary.
Make detailed records: All periodontal assessments and findings should be recorded in a patient’s clinical records, along with details of any discussions with the patient. Even if the treatment plan requires only monitoring and oral hygiene instructions, notes of the discussion and advice given, as well as any follow-up, should be as detailed as possible. An article in BDJ Team provides some useful phrases to include in templates, which should always be personalised (Wadia R, D’Cruz L. Avoiding the pitfalls of dento-legal issues. BDJ Team 2018;5:18091).
Provide written information: Wadia and D’Cruz also suggest using written information leaflets, and if a patient is non-compliant, then it may help to write them a letter explaining the importance of treatment. Ensure these actions are recorded in the patient’s notes.
Manage complaints proactively: Any complaints should be handled quickly and proactively to limit the damage.
At Dental Defence Society, our dento-legal experts can provide timely advice about dealing with complaints and claims regarding periodontal disease. Please contact us for 24/7 support as soon as a case arises.

Dec 31, 2021
On 24th November, the UK Health Security Agency published new guidance for infection prevention and control (IPC) in health and care settings, focusing on seasonal respiratory viruses, especially COVID-19, influenza and respiratory syncytial virus. This guidance supersedes the previous UK IPC COVID-19 guidance.
The IPC Dental Appendix was also updated in line with the guidance. This applies to all areas of dentistry including both NHS dentists and private dental practices. The Chief Dental Officer (CDO) for England, Sara Hurley, subsequently published an updated SOP for dental teams, which has been updated to complement the IPC guidance.
The main change for dentists is the introduction of a risk-based, two-pathway approach. Dental practices and staff should make sure that they are aware of the changes and follow the new guidance to protect themselves and patients.
Key changes to the overall UK IPC guidance
The main changes to the UK IPC guidance include removal of the three COVID-19 specific care pathways (high, medium and low) and addition of a section on the criteria to be applied within the ‘hierarchy of controls’ to further support organisations/services with maximum workplace risk mitigation.
New recommendations to be aware of are:
- Universal use of face masks for staff and face masks/coverings for all patients/visitors within health and care settings over the winter period.
- Physical distancing should be at least 1 metre, increasing whenever feasible to 2 metres across all health and care settings.
- Physical distancing should remain at 2 metres where patients with suspected or confirmed respiratory infection are being cared for or managed.
- Screening, triaging and testing for SARS-CoV-2 should continue over the winter period. Testing for other respiratory pathogens will depend on the health and care setting according to local/country-specific testing strategies/frameworks and data.
New clinical pathways for dental practices
With removal of the three COVID-19 specific care pathways, the new guidance in the Dental Appendix recommends use of a screening tool to determine which of two clinical pathways patients should take within a dental practice.
Non-respiratory pathway (patient has answered NO to all screening questions):
- Complete the appointment applying standard infection control precautions (note: country-specific requirements may be in place for testing prior to aerosol generating procedures [AGPs]).
- Physical distancing should be at least 1 metre in all areas where possible, for example when not providing direct clinical care. Patients may sit in waiting rooms together provided a physical distance of at least 1 metre can be maintained. This should be increased to 2 metres whenever feasible.
- Face coverings are acceptable for patients.
- Dental treatments, both AGP and non-AGP, can go ahead without fallow time.
Respiratory pathway (patient has answered YES to one or more screening questions):
- If possible, based on a clinical assessment, reschedule the appointment until resolution of symptoms, the end of the isolation period or a negative test result.
- Transmission-based precautions (TBP) should be applied in addition to standard infection control precautions. This includes appropriate personal protective equipment (PPE) and respiratory protective equipment (RPE) according to the setting/treatment.
- Patients should be separated, in time or space, from patients on the non-respiratory pathway. Refer to local arrangements as to where treatment should be carried out.
- Provide patients with surgical masks type II or type IIR in place of a universal face covering.
- Physical distancing of at least 2 metres is required.
- For patients undergoing AGPs, TBPs apply and post-AGP downtime is required. Only essential staff necessary to undertake the procedure should be present.
- Carry out any AGP procedures at the end of the day or clinical session to minimise the impact of fallow time on other patients.
Implications of Omicron for IPC measures
With the current surge in COVID-19 cases and spread of the highly transmissible Omicron variant, dentists have questioned whether the new guidance still applies.
Sara Hurley provided an update, in which she wrote: “Dental practices should continue to see patients in line with our infection prevention control guidelines, with the standard operating procedure helping you implement them in practice.”
She added: ”if as new evidence emerges the IPC requirements need to change, the guidance will be updated.”
She also urged dental team members to get their COVID-19 vaccinations and booster. The Department of Health and Social Care has announced that individuals undertaking Care Quality Commission regulated activities in England must be fully vaccinated against COVID-19 by 1st April 2022. This will apply to staff in both NHS and private practices. NHS England has written to all dental practices with more details of the requirement.
The CDO also asked dentists to complete the England Dental Working Patterns Survey from NHS England to help better understand views on the challenges presented by the pandemic and the measures put in place (deadline Sunday 9 January).
Please do not hesitate to contact Dental Defence Society if you need dento-legal support related to infection control precautions.

Nov 10, 2021
Despite the well-known association of smoking with cancer and cardiovascular diseases, about 7m adults in the UK are current smokers. They may not realise that tobacco smoking also damages oral health, being a major risk factor for both oral cancer and periodontal disease.
Dental teams play an important role in prevention of oral cancer and periodontal disease, which includes supporting patients to quit smoking, alongside advice about good oral hygiene and diet. Routine appointments provide opportunities for asking about smoking as well as use of alternative tobacco and nicotine products, such as shisha and e-cigarettes.
Dental practitioners should be aware of such alternative forms of smoking, which are also linked to periodontal disease. For e-cigarettes, the issue is complex as, although not risk-free, they play a role in smoking cessation programmes.
Smoking is a major cause of periodontal disease
Periodontal disease is a leading cause of tooth loss, which can affect patients’ speech, nutrition and quality of life. It is also linked to various systemic diseases.
Family history, poor oral hygiene, stress, and smoking are all important risk factors. A recent systematic review estimated that tobacco smoking increases the risk of periodontitis by 85%. It also increases severity of periodontal disease and diminishes the treatment response.
However, many of the effects of smoking on oral tissues are reversible. Quitting smoking is one of the most important ways in which people can improve their oral health. Strong evidence shows that over time, patients who quit benefit from a reduced risk of periodontitis and tooth loss. The best way to quit is with a combination of specialist support and medication.
E-cigarettes: are they any better for oral health?
On the one hand, e-cigarettes are less harmful than conventional cigarettes and they can help people to quit smoking. In a Cochrane review, more people quit when using nicotine e-cigarettes than when using other nicotine replacement therapies (NRTs). More than 3 million people use e-cigarettes in Great Britain. The vast majority are ex-smokers or dual users, who vape to reduce their need for conventional cigarettes.
On the other hand, vaping is not risk free and non-smokers are not advised to take up vaping. A number of studies and anecdotal reports have raised concerns about deterioration in oral health, accelerated development of caries, and destruction of the periodontium and jaw bone among vapers. But e-cigarettes are a relatively recent innovation and evidence is sparse. Well-conducted, longitudinal studies are needed.
Shisha is not a safer alternative to smoking cigarettes
Shisha (tobacco waterpipe or hookah) is commonly misperceived to be less harmful than conventional smoking. However, shisha smoke contains levels of volatile organic compounds, ultrafine particles, nicotine, and carbon monoxide at least equivalent to cigarette smoke. Incredibly, shisha smokers can inhale over 40 litres of smoke in a single session, much more than from a single cigarette (up to 1 litre).
Like cigarette smokers, shisha smokers are at increased risk of developing oral cancer and periodontal disease and bone loss. As the popularity of shisha is increasing in the UK, especially among younger adults, dentists should ask patients about its use.
What are dental practitioners expected to do?
Dental practitioners are uniquely placed to support their patients in preventing oral cancer and periodontal disease. Public Health England published an updated guideline in September 2021: Delivering better oral health: an evidence-based toolkit for prevention.
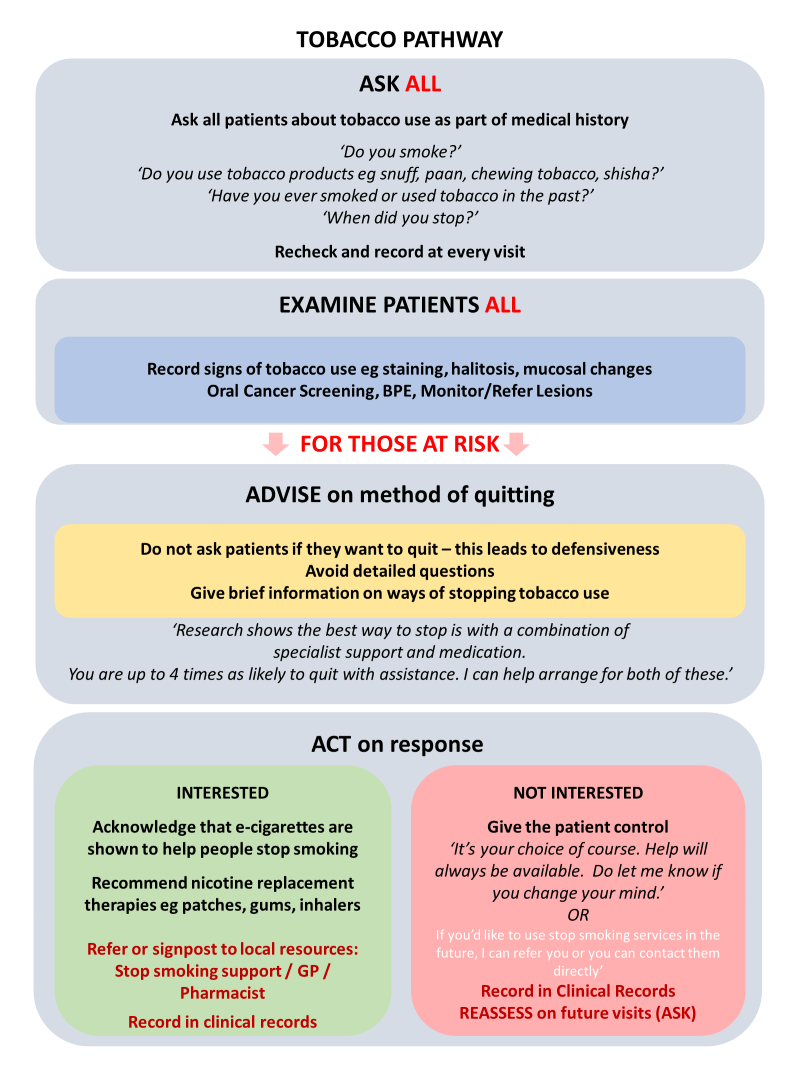
Clinical assessment should include asking patients about use of tobacco and NRTs such as e-cigarettes. It is important to ask about alternative forms of tobacco (e.g. shisha, smokeless, nasal snuff) and use the names of products used locally.
For patients who do smoke, advice can be given about quitting smoking, as outlined in: Very brief advice pathway: 30 second discussion. This Very Brief Advice (VBA) from the dental team can increase a patient’s motivation to quit smoking and double their chances of success.
To avoid creating a defensive reaction, the VBA does not include warning patients about the dangers of smoking or advising them to stop. Instead, dental professionals should refer patients who want to stop to specialist support services where available, or to their GP or pharmacist.
The legal perspective
Further advice can be found in the Healthy gums do matter toolkit from the British Society of Periodontology and Implant Dentistry. This includes a valuable section on legal and ethical perspectives.
The advice emphasises the need to follow guidelines, communicate well with patients about their oral health, and keep detailed records of decisions and reasoning (especially if deviation from the guidelines is deemed to be in the patient’s interest). Following these principals will help in the event of a claim for clinical negligence regarding a patient’s periodontal health.
If you are a member needing dento-legal support for a complaint or claim related to a patient’s oral health, Dental Defence Society is available 24/7 to answer your call and provide advice.

Nov 4, 2021
Dental implants are not really taught at University. Yes, students may be given a 1-2 day course on them, practicing on models, but actual clinical experience is very limited. As such students qualify with little or no regard for dental implant therapy. Moving forward to qualification, only 9% of students surveyed (via a student social media platform) had any intention of learning about dental implants in their careers.
One of the barriers to entry was stated as being indemnity costs. The standard indemnity fee for an associate in the UK appears to vary between £2500 – £5000 with most of the major dental insurance/indemnity providers. If implant placement is added to the policy this can rise to almost £13,000 if sinus lifting is included.
For the average dental associate this is a huge price increase and makes the provision of implant therapy, along with the added costs of equipment, training and time taken to become proficient a large barrier to entry. This explains why implant dentistry is one of the slowest growing areas of dentistry in the UK when compared to facial aesthetics and Invisalign/STO.
What is the justification that indemnity organisations use for such high premiums for those carrying out implant work?
By its very nature, implant dentistry can be the most challenging of all dental modalities. We must be aware of not only the surgical envelope, but also the restorative with many complications being encountered by even the most gifted surgeons on a regular basis.
The UK has no specialist list in implant dentistry, which means those placing implants have varying levels of training. Compared with a specialist Endodontist who has passed standardised exam/approved training pathways, implant surgeons can partake in a 1-day, 1-week or 2-year programme depending on their circumstance. This can make it hard for indemnity organisations to tailor indemnity risks.
As a result, there appears to be a general band which implant surgeons fall into when placing implants. Non sinus placements, and non-graft cases are at a lower banding when compared with complicated bone graft and sinus cases. Sinus cases and full arch cases have a higher level of complication attributed to them compared with simple premolar/molar placements requiring neither.
At DDS (Dental Defence Society) we judge each application for indemnity cover individually. We assess education, experience and competency in implant dentistry before offering a tailor-made indemnity proposal.
When implant work goes wrong either from an integration/function or an aesthetic viewpoint, they can be difficult and time consuming to fix. Senior implant surgeons seem to spend more clinical time treating peri-implant disease or re-doing work which has failed. One of the hardest tasks is attributing blame. Implant dentistry is only provided privately in the UK (except small cases from teaching hospitals) and as such, there is a huge expectation placed upon the work. A failed implant solution does attract a high risk of complaints leading to extra pressure on indemnity organisations to increase premiums for implant work.
Implants surgery can have serious complications such as nerve damage, sinus membrane tears and post-surgical infections. All of these can attract large claims, with certain dental legal firms pursuing implant cases for compensation on a regular basis knowing that these, if successful, can attract large payouts.
So where does the future lie for implant dentistry?
Having a standardised training programme would aim to ‘level up’ all dentists placing implants, making indemnity offers for these individuals potentially less risky. Certain providers are asking for proof of training and judging indemnity based on the quality of the implant teaching received, with those who have achieved post-graduated awards being considered lower risk than those who have not.
Implant dentistry remains one of the most challenging and rewarding areas of dentistry. If we are to maintain a healthy number of skilled implant surgeons in the UK, then more needs to be done to encourage adequate training, and some of the barriers to entry for potential implant surgeons need to be removed.
Please contact DDS for any further information.

Oct 7, 2021
Referrals for oral cancer have fallen dramatically since the start of the pandemic, raising fears that many cases have gone undiagnosed because of disruption to routine dental care. Missed opportunities for early detection mean it is likely that thousands of patients will eventually present with late-stage disease and poor prognosis. They will also require aggressive and complex treatments that diminish their quality of life and add to the burden on the healthcare system.
Now more than ever, dental teams must prioritise the prevention, early detection and rapid referral of oral cancer. They will play a vital role in mitigating the ongoing impact of the pandemic on outcomes for this cancer through performing examinations at every opportunity, recognising when a patient presents with signs and symptoms, and raising awareness.
Increasing burden of oral cancer in the UK
The most recent figures on mouth cancer in the UK align with the global trend, showing an alarming rise in incidence and mortality. The State of Mouth Cancer UK Report 2020/21 reports that last year 8,722 people were diagnosed with mouth cancer and an estimated 2,702 people died from the disease, up 58% and 48%, respectively, from a decade ago.
Early detection and rapid referral for treatment makes a huge difference for patients with oral cancer, boosting survival from 50% to 90%. But even before the pandemic, most patients were diagnosed at a late stage, needing aggressive treatments and experiencing poor clinical outcomes.
Why are outcomes so poor? Patients are often unaware of oral cancer and its symptoms so they seek help late, clinicians do not perform enough soft tissue examinations, and many patients do not attend regular dental appointments – either through choice or because of limited access.
Impact of COVID-19 on oral cancer
The COVID-19 crisis has only worsened the situation by disrupting routine dental care. Although dental practices have re-opened, capacity is still well below pre-COVID levels. While dentists focus on urgent treatments, they may not be checking for signs and symptoms of oral cancer.
According to one of England’s biggest NHS Trusts, referrals fell by 65% after the beginning of lockdown. This suggests that thousands of patients are living with undiagnosed oral cancers and opportunities for early detection are being missed.
The pandemic may also have a long-term impact on the incidence of oral cancer. During lockdowns, some people engaged more often in behaviours that are known risk factors, such as smoking and excess drinking. School closures also interrupted full delivery of vaccination against human papillomavirus (HPV), another important risk factor.
Dental teams have a vital role in improving oral cancer outcomes
A huge effort is needed to stem the rise in cases of oral cancer and improve outcomes for patients. Dental teams will play a leading role by providing:
- Perform intra- and extra-oral examinations at every opportunity, during routine check-ups and treatment appointments. Provide rapid access to an oral examination for patients with suspected lesions who are referred by local GPs or pharmacists.
- Urgently refer patients with suspected lesions to secondary care via the suspected cancer pathway. Have protocols in place and follow the relevant guidance, e.g. from NICE or NHS Scotland.
- Patient education. Raise awareness of oral cancer, associated risk factors, the signs and symptoms and the importance of early detection. Make information available to patients through websites, printed resources and other communications.
- Information on self-examination. Support patients to examine themselves for early signs of oral cancer, with information about how to do this and the symptoms to look out for. Emphasise the importance of reporting symptoms early. The Mouth Cancer Foundation website includes useful information and downloads.
- Support for Mouth Cancer Action Month. Get involved in this campaign run by the Oral Health Foundation each November; resources are available on the website.
- Support for the HPV vaccination campaign. Encourage anyone eligible to have the HPV vaccination when offered it.
Dentists must be vigilant and keep up-to-date
To ensure the best care for patients with oral cancer, it is vital that dental clinicians remain vigilant in checking and referring according to clinical guidelines. From a dento-legal perspective, it is important to keep detailed records, including both positive and negative findings from intra- and extra-oral examinations.
Dentists should maintain an up-to-date knowledge of oral cancer and how to detect it. The BDA provides a valuable oral cancer toolkit, developed in partnership with Cancer Research UK, as well as a number of courses and webinars on the topic. BDA Scotland also offers resources on oral cancer.
If you need advice or dento-legal support related to the treatment of patients with oral cancer, please call our team of experts at Dental Defence Society

Sep 6, 2021
On 6 April 2021, changes to tax law were introduced that dental practice owners and staff should be aware of. The new ‘IR35’ off-payroll working rules are intended to prevent the avoidance of employment tax and national insurance contributions (NICs) by workers treating themselves as self-employed when their actual working practice is consistent with being an employee.
Ahead of the change, there was confusion about what it would mean for the employment status of associate dentists, hygienists and other dental therapists. Many were concerned about inadvertently falling foul of the rules and being subject to additional tax payments, especially as HMRC was seen to increase activity in the dental sector.
Now that the new IR35 rules are in place, be sure you know how and when they apply, and what actions you need to take to ensure compliance.
IR35: how do the rules apply?
Changes to the IR35 off-payroll working rules mean that all public authorities and medium or large-sized private-sector companies are responsible for deciding the employment status of workers. Public sector employers (including NHS dental practices) have long held this responsibility. Now, the rules also apply to private companies meeting two or more of the following conditions:
- annual turnover >£10.2 million
- balance sheet total >£5.1 million
- >50 employees.
In a medium or large private dental practice (or practice group), the responsibility for determining employment status lies with the person engaging the worker, usually the Principal Dentist or practice owner.
If you are an associate dentist or hygienist providing services to a small private dental practice, your own intermediary (usually a limited company) will remain responsible.
Status Determination Statement (SDS) for every contract
If you hold responsibility for determining employment status in a private dental practice, you must prepare an SDS for every worker operating through their own intermediary (even those provided by an agency).
The SDS states the conclusion, with reasons, and is required for each new contract or change in working practice. You must share the SDS with the worker and the person or organisation the contract is with. You are expected to take reasonable care to make an accurate determination and to introduce a process to consider the worker’s views if they disagree.
Keep detailed records. Failure to provide an SDS or take reasonable care could result in the worker’s income tax and NICs becoming your responsibility.
Most associate dentists are self-employed
If you are a dentist employed by a practice, your earnings will be taxed as employment income and subject to Class 1 NICs.
However, if you are an associate dentist, engaged through a standard form of agreement, you are likely to be considered self-employed, even if you operate through an intermediary. Your income is assessable as trading income and you will pay Class 2/4 NICs.
According to James Goldman, writing for the British Dental Association (BDA), it is likely that most associate dentists will continue to be considered self-employed under the new IR35 rules. However, each case should be determined individually.
Goldman says that “for an associate to be self-employed they must:
- Have clinical freedom. They should have the ability to choose their own hours at least to some extent.
- Be involved in complaints against them.
- Be able to affect their income by, for example, providing private treatment.
- Be able to arrange a locum to do work for them.
- Decide what they charge.”
What is the risk for dentists and hygienists?
The risk comes if HMRC decides that your working practice is consistent with that of an employee. This applies even if you are an associate dentist engaged through a standard agreement. Also consider this if you are a hygienist or dental therapist – you may not have the same freedoms and independence as associate dentists so the risk may be increased.
HMRC may challenge your employment status if it finds a discrepancy between your contract and the nature of your working relationship. If you are deemed to be an employee, PAYE and Class 1 NIC would be due.
The risk for the Principal Dentist or practice owner is that they would become liable for the tax and NICs, so contracts are likely to include an indemnity clause to recover those costs.
What actions are required?
Principal Dentists and practice owners are advised to review contracts for all self-employed workers, and to use a standard agreement, such as the BDA model associate agreement. Ensure each contract reflects the true nature of the engagement and prepare an SDS when relevant.
Associate dentists, hygienists and other dental therapists should also review their contracts.
The Check Employment Status for Tax service can help determine if the off-payroll working rules apply. You may want to consult a specialist accountant with knowledge of the dental industry.
If HMRC contact you with questions about employment status, seek advice before you respond.
For any questions about contracts and employment status, please get in touch with our specialist team at Dental Defence Society.
{kind=link}
Recent Comments