
Smoking and periodontal disease
Despite the well-known association of smoking with cancer and cardiovascular diseases, about 7m adults in the UK are current smokers. They may not realise that tobacco smoking also damages oral health, being a major risk factor for both oral cancer and periodontal disease.
Dental teams play an important role in prevention of oral cancer and periodontal disease, which includes supporting patients to quit smoking, alongside advice about good oral hygiene and diet. Routine appointments provide opportunities for asking about smoking as well as use of alternative tobacco and nicotine products, such as shisha and e-cigarettes.
Dental practitioners should be aware of such alternative forms of smoking, which are also linked to periodontal disease. For e-cigarettes, the issue is complex as, although not risk-free, they play a role in smoking cessation programmes.
Smoking is a major cause of periodontal disease
Periodontal disease is a leading cause of tooth loss, which can affect patients’ speech, nutrition and quality of life. It is also linked to various systemic diseases.
Family history, poor oral hygiene, stress, and smoking are all important risk factors. A recent systematic review estimated that tobacco smoking increases the risk of periodontitis by 85%. It also increases severity of periodontal disease and diminishes the treatment response.
However, many of the effects of smoking on oral tissues are reversible. Quitting smoking is one of the most important ways in which people can improve their oral health. Strong evidence shows that over time, patients who quit benefit from a reduced risk of periodontitis and tooth loss. The best way to quit is with a combination of specialist support and medication.
E-cigarettes: are they any better for oral health?
On the one hand, e-cigarettes are less harmful than conventional cigarettes and they can help people to quit smoking. In a Cochrane review, more people quit when using nicotine e-cigarettes than when using other nicotine replacement therapies (NRTs). More than 3 million people use e-cigarettes in Great Britain. The vast majority are ex-smokers or dual users, who vape to reduce their need for conventional cigarettes.
On the other hand, vaping is not risk free and non-smokers are not advised to take up vaping. A number of studies and anecdotal reports have raised concerns about deterioration in oral health, accelerated development of caries, and destruction of the periodontium and jaw bone among vapers. But e-cigarettes are a relatively recent innovation and evidence is sparse. Well-conducted, longitudinal studies are needed.
Shisha is not a safer alternative to smoking cigarettes
Shisha (tobacco waterpipe or hookah) is commonly misperceived to be less harmful than conventional smoking. However, shisha smoke contains levels of volatile organic compounds, ultrafine particles, nicotine, and carbon monoxide at least equivalent to cigarette smoke. Incredibly, shisha smokers can inhale over 40 litres of smoke in a single session, much more than from a single cigarette (up to 1 litre).
Like cigarette smokers, shisha smokers are at increased risk of developing oral cancer and periodontal disease and bone loss. As the popularity of shisha is increasing in the UK, especially among younger adults, dentists should ask patients about its use.
What are dental practitioners expected to do?
Dental practitioners are uniquely placed to support their patients in preventing oral cancer and periodontal disease. Public Health England published an updated guideline in September 2021: Delivering better oral health: an evidence-based toolkit for prevention.
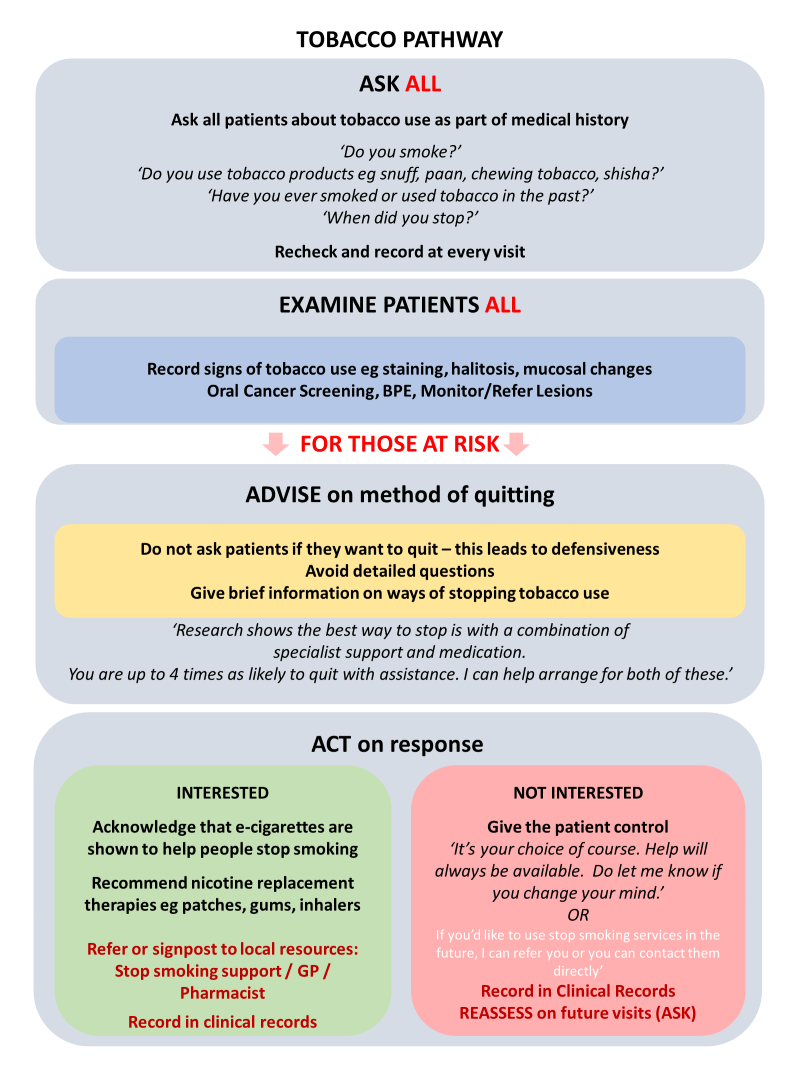
Clinical assessment should include asking patients about use of tobacco and NRTs such as e-cigarettes. It is important to ask about alternative forms of tobacco (e.g. shisha, smokeless, nasal snuff) and use the names of products used locally.
For patients who do smoke, advice can be given about quitting smoking, as outlined in: Very brief advice pathway: 30 second discussion. This Very Brief Advice (VBA) from the dental team can increase a patient’s motivation to quit smoking and double their chances of success.
To avoid creating a defensive reaction, the VBA does not include warning patients about the dangers of smoking or advising them to stop. Instead, dental professionals should refer patients who want to stop to specialist support services where available, or to their GP or pharmacist.
The legal perspective
Further advice can be found in the Healthy gums do matter toolkit from the British Society of Periodontology and Implant Dentistry. This includes a valuable section on legal and ethical perspectives.
The advice emphasises the need to follow guidelines, communicate well with patients about their oral health, and keep detailed records of decisions and reasoning (especially if deviation from the guidelines is deemed to be in the patient’s interest). Following these principals will help in the event of a claim for clinical negligence regarding a patient’s periodontal health.
If you are a member needing dento-legal support for a complaint or claim related to a patient’s oral health, Dental Defence Society is available 24/7 to answer your call and provide advice.

{kind=link}
Recent Comments